The dengue virus affects millions of people every year worldwide, causing large epidemic outbreaks that disrupt people’s lives and severely strain healthcare systems. In the absence of a reliable vaccine against it or an effective treatment to manage the illness in humans, most efforts to combat dengue infections have focused on preventing its vectors, mainly the Aedes aegypti mosquito, from flourishing across the world. These mosquito-control strategies need reliable disease activity surveillance systems to be deployed. Despite significant efforts to estimate dengue incidence using a variety of data sources and methods, little work has been done to understand the relative contribution of the different data sources to improved prediction. Additionally, most work has focused on prediction systems at the national level, rather than at finer spatial resolutions. We develop a methodological framework to assess and compare dengue incidence estimates at the city level and evaluate the performance of a collection of models on 20 different cities in Brazil. The data sources we use towards this end are weekly incidence counts from prior years (seasonal autoregressive terms), weekly-aggregated weather variables, and real-time internet search data. We find that a random forest-based model effectively leverages these multiple data sources and provides robust predictions, while retaining interpretability. For real-time predictions that assume long delays (6-8 weeks) in the availability of epidemiological data, we find that real-time internet search data are the strongest predictors of Dengue incidence, whereas for predictions that assume very short delays (1-2 weeks), short-term and seasonal autocorrelation are dominant as predictors. Despite the difficulties inherent to city-level prediction, our framework achieves meaningful and actionable estimates across cities with different characteristics.
Objectives: To create a machine-learning model identifying potentially avoidable blood draws for serum potassium among pediatric patients following cardiac surgery. Design: Retrospective cohort study. Setting: Tertiary-care center. Patients: All patients admitted to the cardiac ICU at Boston Children’s Hospital between January 2010 and December 2018 with a length of stay greater than or equal to 4 days and greater than or equal to two recorded serum potassium measurements. Interventions: None. Measurements and Main Results: We collected variables related to potassium homeostasis, including serum chemistry, hourly potassium intake, diuretics, and urine output. Using established machine-learning techniques, including random forest classifiers, and hyperparameter tuning, we created models predicting whether a patient’s potassium would be normal or abnormal based on the most recent potassium level, medications administered, urine output, and markers of renal function. We developed multiple models based on different age-categories and temporal proximity of the most recent potassium measurement. We assessed the predictive performance of the models using an independent test set. Of the 7,269 admissions (6,196 patients) included, serum potassium was measured on average of 1 (interquartile range, 0–1) time per day. Approximately 96% of patients received at least one dose of IV diuretic and 83% received a form of potassium supplementation. Our models predicted a normal potassium value with a median positive predictive value of 0.900. A median percentage of 2.1% measurements (mean 2.5%; interquartile range, 1.3–3.7%) was incorrectly predicted as normal when they were abnormal. A median percentage of 0.0% (interquartile range, 0.0–0.4%) critically low or high measurements was incorrectly predicted as normal. A median of 27.2% (interquartile range, 7.8–32.4%) of samples was correctly predicted to be normal and could have been potentially avoided. Conclusions: Machine-learning methods can be used to predict avoidable blood tests accurately for serum potassium in critically ill pediatric patients. A median of 27.2% of samples could have been saved, with decreased costs and risk of infection or anemia.
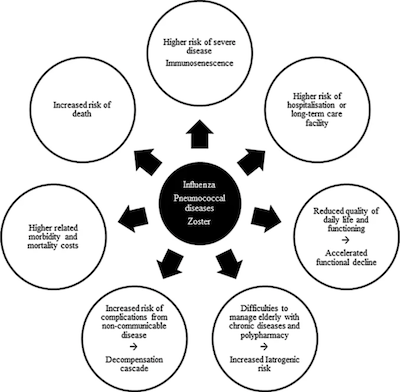
Despite immunisation being one of the greatest medical success stories of the twentieth century, there is a growing lack of confidence in some vaccines. Improving communication about the direct benefits of vaccination as well as its benefits beyond preventing infectious diseases may help regain this lost confidence. A conference was organised at the Fondation Merieux in France to discuss what benefits could be communicated and how innovative digital initiatives can used for communication. During this meeting, a wide range of indirect benefits of vaccination were discussed. For example, influenza vaccination can reduce hospitalisations and deaths in older persons with diabetes by 45% and 38%, respectively, but the link between influenza and complications from underlying chronic non-communicable diseases such as diabetes is frequently underestimated. Vaccination can reduce antimicrobial resistance (AMR), which is growing, by reducing the incidence of infectious disease (though direct and indirect or herd protection), by reducing the number of circulating AMR strains, and by reducing the need for antimicrobial use. Disease morbidity and treatment costs in the elderly population are likely to rise substantially, with the ageing global population. Healthy ageing and life-course vaccination approaches can reduce the burden of vaccine-preventable diseases, such as seasonal influenza and pneumococcal diseases, which place a significant burden on individuals and society, while improving quality of life. Novel disease surveillance systems based on information from Internet search engines, mobile phone apps, social media, cloud-based electronic health records, and crowd-sourced systems, contribute to improved awareness of disease burden. Examples of the role of new techniques and tools to process data generated by multiple sources, such as artificial intelligence, to support vaccination programmes, such as influenza and dengue, were discussed. The conference participants agreed that continual efforts are needed from all stakeholders to ensure effective, transparent communication of the full benefits and risks of vaccination.
Aggregated mobility data could help fight COVID-19 Buckee CO, Balsari S, Chan J, Crosas M, Dominici F, Gasser U, Grad YH, Grenfell B, Halloran ME, Kraemer MUG, et al. Science. 2020;368 (6487) :145-146.
Abstract
As the coronavirus disease 2019 (COVID-19) epidemic worsens, understanding the effectiveness of public messaging and large-scale social distancing interventions is critical. The research and public health response communities can and should use population mobility data collected by private companies, with appropriate legal, organizational, and computational safeguards in place. When aggregated, these data can help refine interventions by providing near real-time information about changes in patterns of human movement.
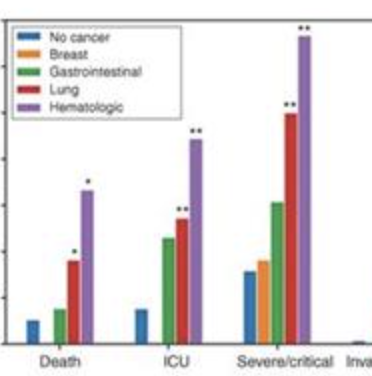
The novel COVID-19 outbreak has affected more than 200 countries and territories as of March 2020. Given that patients with cancer are generally more vulnerable to infections, systematic analysis of diverse cohorts of patients with cancer affected by COVID-19 is needed. We performed a multicenter study including 105 patients with cancer and 536 age-matched noncancer patients confirmed with COVID-19. Our results showed COVID-19 patients with cancer had higher risks in all severe outcomes. Patients with hematologic cancer, lung cancer, or with metastatic cancer (stage IV) had the highest frequency of severe events. Patients with nonmetastatic cancer experienced similar frequencies of severe conditions to those observed in patients without cancer. Patients who received surgery had higher risks of having severe events, whereas patients who underwent only radiotherapy did not demonstrate significant differences in severe events when compared with patients without cancer. These findings indicate that patients with cancer appear more vulnerable to SARS-CoV-2 outbreak.
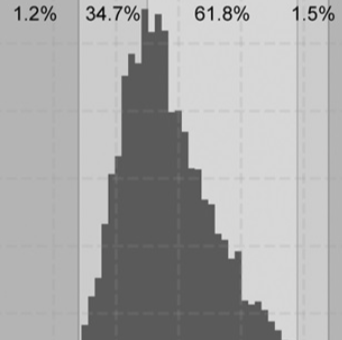
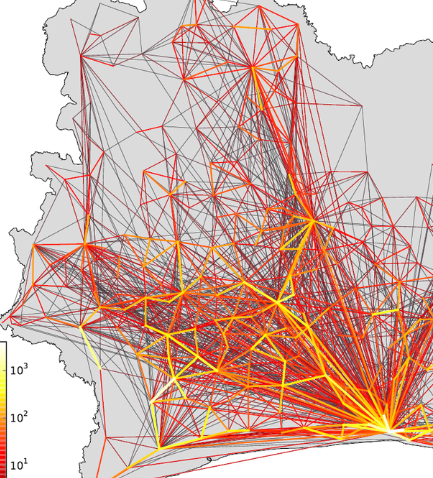
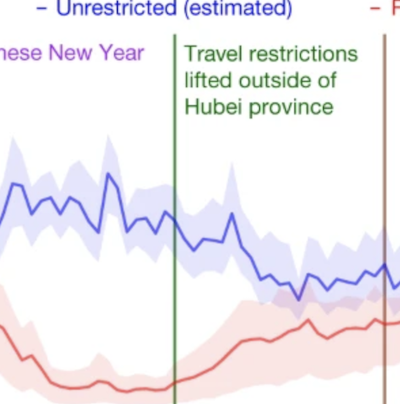
On 11 March 2020, the World Health Organization (WHO) declared coronavirus disease 2019 (COVID-19) a pandemic1. The strategies based on non-pharmaceutical interventions that were used to contain the outbreak in China appear to be effective2, but quantitative research is still needed to assess the efficacy of non-pharmaceutical interventions and their timings3. Here, using epidemiological data on COVID-19 and anonymized data on human movement4,5, we develop a modelling framework that uses daily travel networks to simulate different outbreak and intervention scenarios across China. We estimate that there were a total of 114,325 cases of COVID-19 (interquartile range 76,776–164,576) in mainland China as of 29 February 2020. Without non-pharmaceutical interventions, we predict that the number of cases would have been 67-fold higher (interquartile range 44–94-fold) by 29 February 2020, and we find that the effectiveness of different interventions varied. We estimate that early detection and isolation of cases prevented more infections than did travel restrictions and contact reductions, but that a combination of non-pharmaceutical interventions achieved the strongest and most rapid effect. According to our model, the lifting of travel restrictions from 17 February 2020 does not lead to an increase in cases across China if social distancing interventions can be maintained, even at a limited level of an on average 25% reduction in contact between individuals that continues until late April. These findings improve our understanding of the effects of non-pharmaceutical interventions on COVID-19, and will inform response efforts across the world.
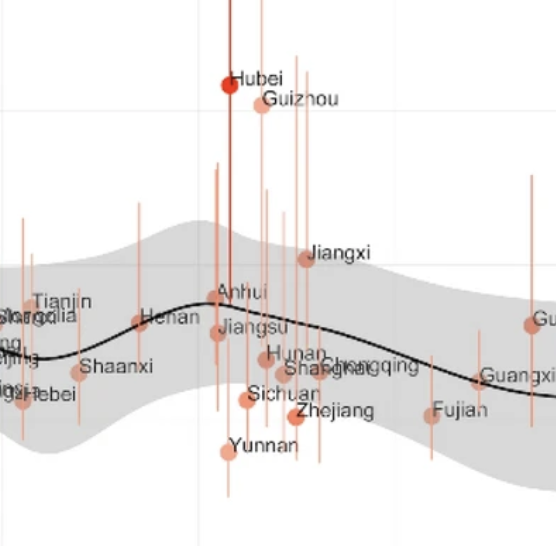
First identified in Wuhan, China, in December 2019, a novel coronavirus (SARS-CoV-2) has affected over 16,800,000 people worldwide as of July 29, 2020 and was declared a pandemic by the World Health Organization on March 11, 2020. Influenza studies have shown that influenza viruses survive longer on surfaces or in droplets in cold and dry air, thus increasing the likelihood of subsequent transmission. A similar hypothesis has been postulated for the transmission of COVID-19, the disease caused by SARS-CoV-2. It is important to propose methodologies to understand the effects of environmental factors on this ongoing outbreak to support decision-making pertaining to disease control. Here, we examine the spatial variability of the basic reproductive numbers of COVID-19 across provinces and cities in China and show that environmental variables alone cannot explain this variability. Our findings suggest that changes in weather (i.e., increase of temperature and humidity as spring and summer months arrive in the Northern Hemisphere) will not necessarily lead to declines in case counts without the implementation of drastic public health interventions.
Over the past two decades, widespread adoption of mobile phone technology has facilitated the real-time acquisition of individual-level data on human behaviour. Mobile technologies have helped to improve geographical navigation, facilitated the exchange of goods and money, accelerated information transfer, and strengthened predictions for the spread of infectious diseases.1, 2, 3. The rise of portable health-monitoring devices has also allowed individuals to track their vital signs and sleep patterns, generating a trove of information to monitor population health.
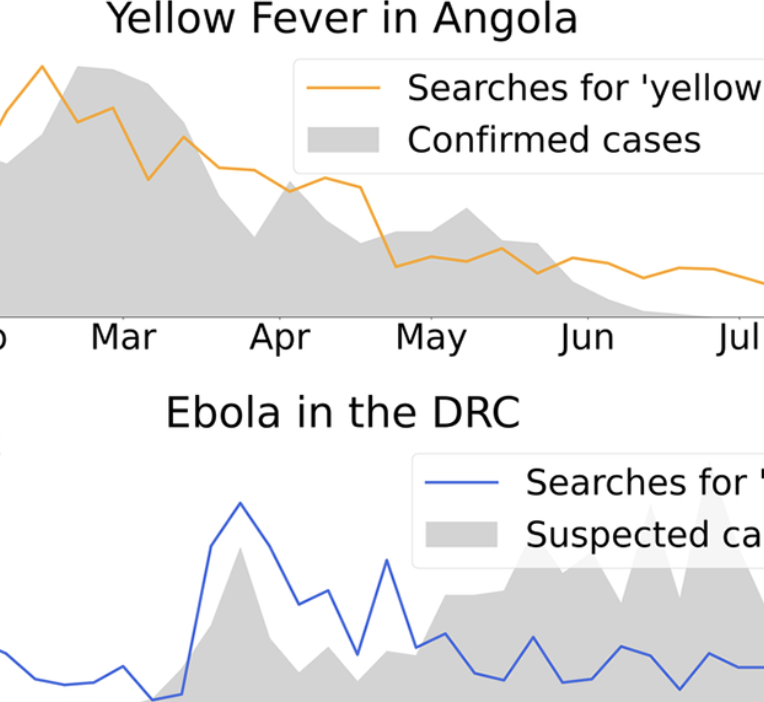
Understanding the behavior of emerging disease outbreaks in, or ahead of, real-time could help healthcare officials better design interventions to mitigate impacts on affected populations. Most healthcare-based disease surveillance systems, however, have significant inherent reporting delays due to data collection, aggregation, and distribution processes. Recent work has shown that machine learning methods leveraging a combination of traditionally collected epidemiological information and novel Internet-based data sources, such as disease-related Internet search activity, can produce meaningful “nowcasts” of disease incidence ahead of healthcare-based estimates, with most successful case studies focusing on endemic and seasonal diseases such as influenza and dengue. Here, we apply similar computational methods to emerging outbreaks in geographic regions where no historical presence of the disease of interest has been observed. By combining limited available historical epidemiological data available with disease-related Internet search activity, we retrospectively estimate disease activity in five recent outbreaks weeks ahead of traditional surveillance methods. We find that the proposed computational methods frequently provide useful real-time incidence estimates that can help fill temporal data gaps resulting from surveillance reporting delays. However, the proposed methods are limited by issues of sample bias and skew in search query volumes, perhaps as a result of media coverage.
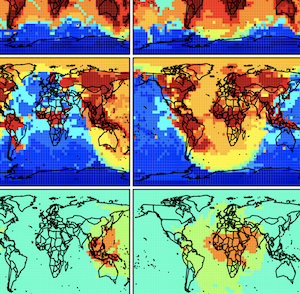
The major computational bottleneck in atmospheric chemistry models is the numerical integration of the stiff coupled system of kinetic equations describing the chemical evolution of the system as defined by the model chemical mechanism (typically over 100 coupled species). We present an adaptive method to greatly reduce the computational cost of that numerical integration in global 3-D models while maintaining high accuracy. Most of the atmosphere does not in fact require solving for the full chemical complexity of the mechanism, so considerable simplification is possible if one can recognize the dynamic continuum of chemical complexity required across the atmospheric domain. We do this by constructing a limited set of reduced chemical mechanisms (chemical regimes) to cover the range of atmospheric conditions and then pick locally and on the fly which mechanism to use for a given grid box and time step on the basis of computed production and loss rates for individual species. Application to the GEOS-Chem global 3-D model for oxidant–aerosol chemistry in the troposphere and stratosphere (full mechanism of 228 species) is presented. We show that 20 chemical regimes can largely encompass the range of conditions encountered in the model. Results from a 2-year GEOS-Chem simulation shows that our method can reduce the computational cost of chemical integration by 30 %–40 % while maintaining accuracy better than 1 % and with no error growth. Our method retains the full complexity of the original chemical mechanism where it is needed, provides the same model output diagnostics (species production and loss rates, reaction rates) as the full mechanism, and can accommodate changes in the chemical mechanism or in model resolution without having to reconstruct the chemical regimes.
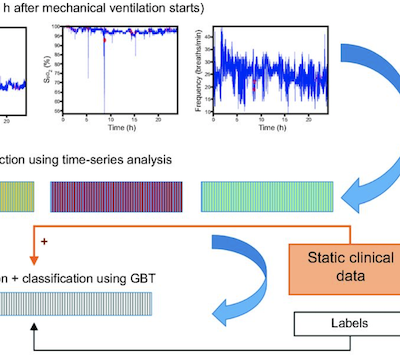
BACKGROUND: Bedside monitors in the ICU routinely measure and collect patients' physiologic data in real time to continuously asess the health status of patients who are critically ill. With the advent of increased computational power and the ability to store and rapidly process big data sets in recent years, these physiologic data show promise in identifying specific outcomes and/or events during patients' ICU hospitalization. METHODS: We introduced a methodology designed to automatically extract information from continuous-in-time vital sign data collected from bedside monitors to predict if a patient will experience a prolonged stay (length of stay) on mechanical ventilation, defined as >4 d, in a pediatric ICU. RESULTS: Continuous-in-time vital signs information and clinical history data were retrospectively collected for 284 ICU subjects from their first 24 h on mechanical ventilation from a medical-surgical pediatric ICU at Boston Children's Hospital. Multiple machine learning models were trained on multiple subsets of these subjects to predict the likelihood that each of these subjects would experience a long stay. We evaluated the predictive power of our models strictly on unseen hold-out validation sets of subjects. Our methodology achieved model performance of >83% (area under the curve) by using only vital sign information as input, and performances of 90% (area under the curve) by combining vital sign information with subjects' static clinical data readily available in electronic health records. We implemented this approach on 300 independently trained experiments with different choices of training and hold-out validation sets to ensure the consistency and robustness of our results in our study sample. The predictive power of our approach outperformed recent efforts that used deep learning to predict a similar task. CONCLUSIONS: Our proposed workflow may prove useful in the design of scalable approaches for real-time predictive systems in ICU environments, exploiting real-time vital sign information from bedside monitors. (ClinicalTrials.gov registration NCT02184208.)
BackgroundThe rapid increase of bacterial antibiotic resistance could soon render our most effective method to address infections obsolete. Factors influencing pathogen resistance prevalence in human populations remain poorly described, though temperature is known to contribute to mechanisms of spread.
AimTo quantify the role of temperature, spatially and temporally, as a mechanistic modulator of transmission of antibiotic resistant microbes.
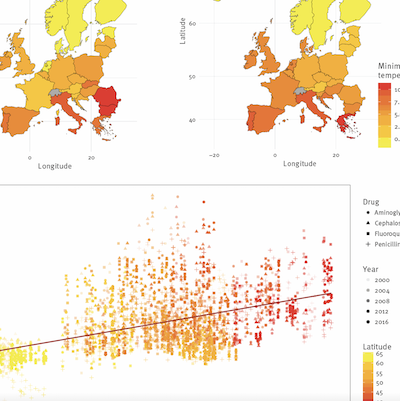
MethodsAn ecologic analysis was performed on country-level antibiotic resistance prevalence in three common bacterial pathogens across 28 European countries, collectively representing over 4 million tested isolates. Associations of minimum temperature and other predictors with change in antibiotic resistance rates over 17 years (2000–2016) were evaluated with multivariable models. The effects of predictors on the antibiotic resistance rate change across geographies were quantified.
ResultsDuring 2000–2016, for Escherichia coli and Klebsiella pneumoniae, European countries with 10°C warmer ambient minimum temperatures compared to others, experienced more rapid resistance increases across all antibiotic classes. Increases ranged between 0.33%/year (95% CI: 0.2 to 0.5) and 1.2%/year (95% CI: 0.4 to 1.9), even after accounting for recognised resistance drivers including antibiotic consumption and population density. For Staphylococcus aureus a decreasing relationship of −0.4%/year (95% CI: −0.7 to 0.0) was found for meticillin resistance, reflecting widespread declines in meticillin-resistant S. aureus across Europe over the study period.
ConclusionWe found evidence of a long-term effect of ambient minimum temperature on antibiotic resistance rate increases in Europe. Ambient temperature might considerably influence antibiotic resistance growth rates, and explain geographic differences observed in cross-sectional studies. Rising temperatures globally may hasten resistance spread, complicating mitigation efforts. METHODS: We introduced a methodology designed to automatically extract information from continuous-in-time vital sign data collected from bedside monitors to predict if a patient will experience a prolonged stay (length of stay) on mechanical ventilation, defined as >4 d, in a pediatric ICU. RESULTS: Continuous-in-time vital signs information and clinical history data were retrospectively collected for 284 ICU subjects from their first 24 h on mechanical ventilation from a medical-surgical pediatric ICU at Boston Children's Hospital. Multiple machine learning models were trained on multiple subsets of these subjects to predict the likelihood that each of these subjects would experience a long stay. We evaluated the predictive power of our models strictly on unseen hold-out validation sets of subjects. Our methodology achieved model performance of >83% (area under the curve) by using only vital sign information as input, and performances of 90% (area under the curve) by combining vital sign information with subjects' static clinical data readily available in electronic health records. We implemented this approach on 300 independently trained experiments with different choices of training and hold-out validation sets to ensure the consistency and robustness of our results in our study sample. The predictive power of our approach outperformed recent efforts that used deep learning to predict a similar task. CONCLUSIONS: Our proposed workflow may prove useful in the design of scalable approaches for real-time predictive systems in ICU environments, exploiting real-time vital sign information from bedside monitors. (ClinicalTrials.gov registration NCT02184208.)